What is Endometriosis?
So I’ve talked a lot about egg retrievals and the meds that go with them. Let’s switch gears for a sec and talk about something that affects way more people than you’d think: endometriosis.
Endometriosis shows up in about ~10% of women globally (and 30%-50% of women if you’re looking just those with infertility). Basically, tissue that’s only supposed to grow inside your uterus decides to be a rebel and set up camp outside, in places like the lining of your abdomen (aka the peritoneum).
And when that happens? Hello, painful periods, pelvic pain, and infertility. If you’re trying to get pregnant, it makes things really tough because the environment isn’t exactly baby-friendly.
Okay, But How Do We Fix It?
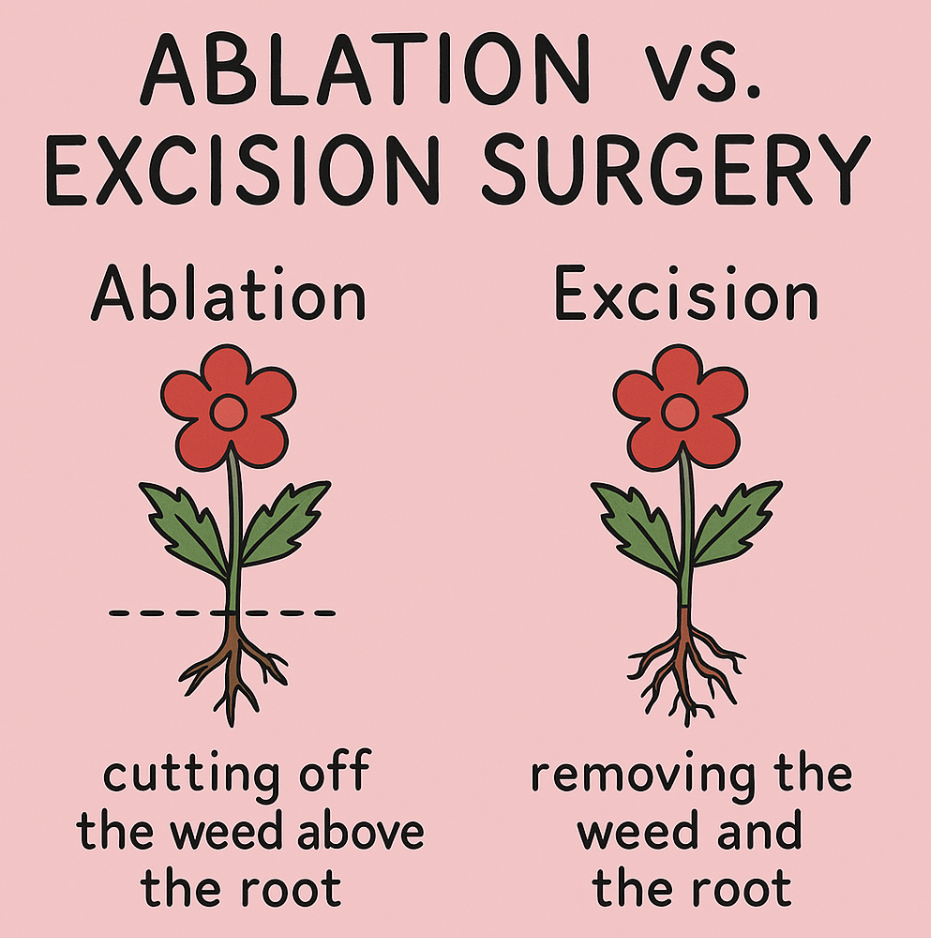
There are two main surgical approaches: ablative therapy and excision surgery.
Excision Surgery
This is the gold standard. Instead of just burning the surface, the surgeon cuts the tissue out completely, roots and all. This makes recurrence way less likely. In fact, excision has an incredibly low risk of the endo coming back. It’s like finally pulling that stubborn dandelion out by the root. Satisfying.
Ablative Therapy
Picture this: the surgeon goes in, makes a few tiny incisions, and then zaps the endo tissue with heat to burn it off. Sounds good, right? Well, yes… until it grows back. Think of it like plucking weeds from your garden but leaving the roots behind. Spoiler: the weeds always return.
So Why Doesn’t Everyone Just Get Excision?
Two words: time and training. Excision surgery is more complex, takes longer, and not every doctor is trained to do it. Unfortunately, that means a lot of patients get stuck with ablation because it’s “easier.” Convenient for the doctor? Sure. Better for the patient long-term? Not really.
At the Jacksonville Center for Reproductive Medicine (JCRM), though, excision is the standard. Every patient with endo gets it, no shortcuts. And here’s the kicker: research shows that having excision surgery before IVF can actually boost your chances of a live birth. Win-win.
Real Talk
Endometriosis is brutal, physically, emotionally, and especially if you’re trying to grow your family. But knowing the difference between treatments (and advocating for excision when possible) can change everything.
I even published an abstract on this exact topic (linked here if you want to nerd out). But if you take away one thing from this post, let it be this: don’t settle for just burning the weed when you could pull it out completely.
